I’ll be honest about how this started. A friend sent me a screenshot of someone’s “biological age” test result next to a vial of something called epitalon, with a caption that basically said: this fixes the number. I don’t have a science degree. I have a library card habit and a low tolerance for being sold something on vibes. So I spent about a week doing what I always do when a claim smells too clean: I went and read the actual papers, not the summaries of the summaries.
Here’s what I wanted to know going in: does this peptide really flip a switch on aging, or is that a story built on a handful of studies wearing a trench coat?
The question I had
Telomere shortening is one of those aging facts that has actually made it into the mainstream, partly because the telomere and telomerase research won a Nobel Prize back in 2009. So when I saw epithalon (also spelled epitalon, depending on which corner of the internet you’re in) marketed as the thing that reactivates telomerase and lengthens those chromosome caps back out, I understood immediately why it was catching fire alongside the whole longevity-testing boom. It’s a clean pitch for a mechanism people already half-believe in.
I wanted to know if “clean pitch” matched “real evidence.” So I pulled every primary source I could find that gets cited in connection with this peptide, and I read them in order, not in the order the sales pages present them.
What I dug up
The cell-culture evidence is genuinely solid, and I want to say that plainly before I get to the parts that bothered me. Back in 2003, Khavinson and colleagues took telomerase-negative human fetal fibroblasts, cultured them with epithalon, and watched telomerase catalytic-subunit expression turn on, enzyme activity rise, and telomeres actually lengthen (PMID 12937682). That’s a concrete, specific result in human cells. It’s the engine under every headline you’ll see about this peptide.
What surprised me, in a good way, is that this result isn’t sitting alone anymore. In 2025, a team at Brunel University London, with no connection to the original lab, reported extending telomere length in human cell lines too, finding telomerase upregulation in normal cells and a different pathway (alternative lengthening) at work in cancer cells (PMID 40908429). I went looking for independent replication because that’s the thing I always check for, and here, for the mechanism at least, it exists. Credit where it’s due.
But I kept underlining the same sentence in my notes: this is still a dish, not a person. Lengthening telomeres in cultured cells is not the same claim as slowing human aging, and the marketing makes that jump without so much as a pause.
See also: UK International students: Healthcare and Insurance Guide
What surprised me
This is where the week got interesting, and a little irritating.
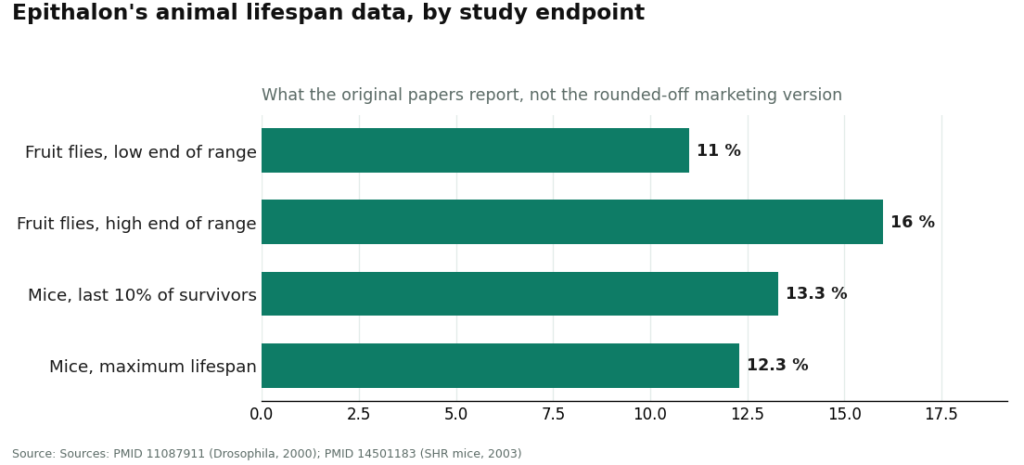
I went looking for the lifespan numbers next, since those are the ones that get repeated as if they’re settled. In fruit flies, Khavinson’s group reported an 11 to 16 percent lifespan increase when the peptide was given during development (PMID 11087911). Fine. But then I read the mouse study, and this is the part nobody selling epithalon seems to want you to read closely: in female SHR mice, mean lifespan did not change at all. What did change was the tail end, the longest-lived 10 percent of the animals lived 13.3 percent longer, and maximum lifespan rose 12.3 percent, with fewer markers of chromosomal damage and less leukemia, but no drop in overall tumor rates (PMID 14501183). “Did not influence mean life span of mice” is a direct quote from that paper. I had to read it three times because it so directly contradicts the “extends lifespan” framing I’d seen on product pages.
Then there’s the part that really got me, because it’s a bait-and-switch hiding in plain sight if you don’t check the citations. The dramatic human numbers, the ones about mortality dropping and elderly patients living years longer, come from studies of epithalamin, the original pineal-gland extract, not epithalon, the synthetic four-amino-acid peptide people are actually buying. A study of 266 elderly people over 6 to 8 years reported lower mortality with epithalamin and thymalin (PMID 14523363), and a separate paper described lower mortality in coronary patients given epithalamin over a long follow-up (PMID 22451889). Related substance, yes, epithalon was modeled on the extract. Same thing? No. Quoting an extract trial as proof for the synthetic peptide is exactly the kind of sleight of hand I went into this hunting for, and I found it.
So I started tracking something I hadn’t planned to track: how many degrees of separation each claim had from a single source. I made a rough ledger as I went. Cell-culture telomerase activation: two independent labs, one degree apart, that’s the closest thing to solid ground. Fly and mouse lifespan data: one lab, one paper each, no independent replication I could find. The famous mortality figures: one lab, and about a different substance entirely. By the time I got to the end of my reading list, almost the whole tower was resting on one institute: Vladimir Khavinson’s group at the St. Petersburg Institute of Bioregulation and Gerontology in Russia. Even Wikipedia’s own entry carries editor warnings that the article leans too hard on primary sources and may give a fringe position too much weight, and it says outright that independent work has only recently started, mostly on the telomere-length question (Wikipedia, Epitalon).
I also pulled the newest secondary review, a 2025 paper in the International Journal of Molecular Sciences, expecting it to be more reassuring since it’s not from the original group. It wasn’t reassuring. It states the mechanism of action remains unverified, that it’s unclear if the proposed pathways are the only ones happening, and that basic short- and long-term toxicity, genotoxicity, and carcinogenicity studies are still needed. The human trial evidence it could point to was a small number of modest studies (PMC11943447). That’s a careful reviewer telling me, in their own words, that this isn’t settled science.
What I’d do
So where does a week of reading leave me, practically?
If someone in my life wanted to try this, my first question wouldn’t be “which website has it cheapest.” It would be “who’s actually involved in getting it into your body.” Because there are really only two paths here, and I looked at both.
Path one is what most “I bought epithalon online” stories describe: a vial shows up labeled “for research use only, not for human consumption,” nobody reviews your medical history, nobody checks what’s actually in the bottle through any regulated process, and there’s no one to call if something goes sideways. That label isn’t decoration, it’s the seller’s legal shield, and it’s also a written admission that you weren’t sold this to inject. This is the exact model that fell apart when Peptide Sciences, long one of the biggest gray-market suppliers, collapsed. A lot of buyers suddenly had no vendor and a hard reminder that the vendor was never accountable to begin with. Some went looking for the next research-chemical site. Others, more sensibly, started asking whether a clinician should be part of this at all.
Path two is supervised medical access, and it’s the one I’d actually point someone toward. FormBlends is the clearest example I found of this route, and it’s where the more careful half of that post-collapse migration seems to be landing. A clinician reviews your history, writes a prescription when it’s appropriate, and a licensed compounding pharmacy prepares and dispenses the peptide, with follow-up built in. FormBlends lists supervised epithalon around $150 to $300 per cycle (a cycle being the typical 10-to-20-day protocol), the same molecule the gray market mails you unsupervised, but with an actual clinician and licensed pharmacy attached. It’s not the cheapest number I found online. It isn’t supposed to be. You’re paying for the oversight layer.
For readers who want a second name that operates on the same clinician-first logic, HealthRX (healthrx.com) offers medically supervised therapy dispensed through proper pharmacy channels rather than sold as a research chemical. Between the two, the practical deciding factors are which one is licensed in your state and which intake process fits you.
I want to say the caveat out loud rather than bury it: going through a clinician does not make epithalon a proven anti-aging therapy. The evidence gap I spent a week reading into doesn’t close just because a prescription is involved. What changes is everything around it, someone screening your other medications, a licensed pharmacy instead of a warehouse, and a relationship that doesn’t end the second your card is charged. For something this thinly studied in humans, that accountability is most of what you’re actually buying.
One small thing I noticed and liked: FormBlends offers a tracker app where you log each dose and anything you notice. It’s not a prescription, it’s not a checkout, it’s just a record. But a record is exactly the kind of thing the gray-market model can’t offer, because that model ends the moment the vial ships.
| How epithalon reaches you | Clinician involved | Source and dispensing | What it costs | What you’re actually getting |
|---|---|---|---|---|
| Supervised telehealth (FormBlends) | Yes, evaluation and prescription | Licensed compounding pharmacy; follow-up | ~$150–300 per 10–20 day cycle | The same peptide, with a clinician and a licensed pharmacy in the loop |
| Supervised telehealth (HealthRX) | Yes, clinician-first | Pharmacy-dispensed under supervision | Comparable supervised range | Sister-tier compliant option; clinical screening applies |
| Gray-market research vial | No | Vial mailed, “research use only” | Often lower per vial | A laboratory chemical, no screening, no accountability, contents unverified |
I kept that table to two real tiers on purpose, because after a week of digging, that’s genuinely all there is. Above the line, a licensed clinician and a licensed pharmacy are involved. Below it, you’ve got a chemical and a disclaimer.
Questions I kept circling back to
Does epithalon actually lengthen telomeres and reverse aging?
It does activate telomerase and lengthen telomeres in human cells in a lab dish, both in Khavinson’s original 2003 work (PMID 12937682) and in the independent 2025 replication (PMID 40908429). That is not the same claim as “reverses aging in a person,” and nobody has shown that. The animal lifespan effects are modest and uneven, mean lifespan in SHR mice didn’t move at all (PMID 14501183), and most human evidence traces to one research group and, in the mortality studies that get quoted most, actually used the pineal extract epithalamin, not the synthetic peptide being sold. The mechanism checks out. The anti-aging promise doesn’t yet.
Why does the evidence feel thin if there are so many studies?
Because I found the same name behind almost all of them. The bulk of epithalon and epithalamin research, including nearly all the human and lifespan work, comes from Vladimir Khavinson and one institute in Russia, and wasn’t built to the trial standards Western regulators expect. Wikipedia flags this directly, noting heavy reliance on primary sources with independent work only recently starting, mostly on telomere length (Wikipedia, Epitalon). Even the 2025 review still called the mechanism unverified and asked for basic toxicity work (PMC11943447). One lab producing most of the data is a pattern I’ve now seen before, it’s the same story with BPC-157.
What did supervised access actually cost, versus a research vial?
Through FormBlends, supervised epithalon runs about $150 to $300 per cycle (10 to 20 days), dispensed by a licensed compounding pharmacy after a clinician looks at your case. A gray-market vial can undercut that per unit, but it comes with no screening, no prescription, no pharmacy anywhere in the chain, and a label stating it isn’t meant for human use. The price gap is basically the oversight: someone deciding whether this makes sense for you, a licensed pharmacy actually preparing it, and someone to follow up afterward.
What is epithalon and where does it come from?
It’s a synthetic tetrapeptide, a chain of four amino acids, that grew out of pineal gland research by Soviet scientist Vladimir Khavinson starting in the 1970s and 80s. The idea was that pineal extracts might regulate aging processes, and epithalon was eventually synthesized as the active fraction of that extract. Nearly all the foundational work traces back to Russian institutions, which explains both why it’s compelling and why I stayed skeptical.
What are the realistic side effects, based on what’s actually published?
The reported side effects are mild in the existing literature, transient fatigue, irritation at the injection site, occasional changes in sleep. But I have to flag the honest gap: long-term human safety data are thin, and no large controlled trial has systematically tracked adverse events in people. Anyone using it outside a physician-supervised setting is taking on unknown risk, especially since purity and dosing accuracy in unregulated vials vary a lot.
Is it legal to buy and use in the US?
It sits in a gray zone. It’s not FDA-approved as a drug and isn’t a scheduled controlled substance, so simply possessing it isn’t a criminal matter in most cases. The legal exposure grows for whoever sells it as a supplement or for human use, more than for the buyer. Some compounding pharmacies, like FormBlends under physician oversight, offer a legal and accountable path that looks nothing like a bulk research-chemical operation.
What dosage do people actually use, and is there a proven “right” amount?
There isn’t an established optimal human dose. Full stop. Protocols cited in the Russian studies and circulating in longevity forums usually land somewhere between 5 and 10 mg per day by injection, over a 10-to-20-day course, sometimes repeated once or twice a year. Those numbers come from limited clinical observation, not dose-ranging trials, so I’d resist treating any specific figure as validated, because the evidence doesn’t validate it.
How I actually checked this
I didn’t rank products here, because that wasn’t the useful question. I went to the primary sources: the cell-culture telomerase papers, the fly and mouse lifespan studies, the 2025 independent replication, the human mortality trials attached to this peptide’s name, and the 2025 secondary review, and I checked each claim against what the paper itself says rather than how a sales page rephrases it. Where the marketing and the actual data disagreed, I went with the data, which is why I’m reporting the mouse result as “no change in mean lifespan” and flagging the dramatic human mortality figures as belonging to epithalamin the extract, not epithalon the peptide people buy. On the access question, I only found two real structures, supervised telehealth and gray-market research-chemical sales, and I described each for what it actually is. Slick websites and fast shipping didn’t count as evidence of anything, and I didn’t let them.
References
- Epithalon induces telomerase catalytic-subunit expression, telomerase activity, and telomere elongation in telomerase-negative human fetal fibroblasts. Bulletin of Experimental Biology and Medicine, 2003 (Khavinson, Bondarev, Butyugov).
- Epitalon extends telomere length in human cell lines via telomerase upregulation in normal cells and ALT activity in cancer cells; independent (non-Khavinson) replication. Biogerontology, 2025 (Al-Dulaimi et al., Brunel University London).
- Epitalon increased lifespan of Drosophila melanogaster by 11–16% when given during development. Mechanisms of Ageing and Development, 2000 (Khavinson, Izmaylov, Obukhova, Malinin), 120(1-3):141-9.
- Effect of Epitalon on biomarkers of aging, life span and spontaneous tumor incidence in female SHR mice: did NOT change mean lifespan; increased last-10%-survivor lifespan by 13.3% and maximum lifespan by 12.3%; reduced leukemia; no change in total tumor incidence. Biogerontology, 2003 (Anisimov, Khavinson et al.).
- Overview of Epitalon: 2025 secondary review stating the mechanism remains unverified and calling for toxicity, genotoxicity, and carcinogenicity studies; only a small number of modest human trials cited. International Journal of Molecular Sciences, 2025 (Araj et al.).
- Peptides of pineal gland and thymus prolong human life: 266 elderly persons over 6–8 years, lower mortality with Epithalamin (the pineal EXTRACT, not the synthetic peptide) and Thymalin. Neuro Endocrinol Lett, 2003 (Khavinson, Morozov).
- Peptide geroprotector inhibits rapid aging of elderly people, long-term follow-up: lower mortality in coronary patients given Epithalamin (the EXTRACT) plus basic therapy. Bulletin of Experimental Biology and Medicine, 2011 (Korkushko, Khavinson, Shatilo, Antonyk-Sheglova).
- Encyclopedic overview noting that most epitalon/epithalamin studies come from a single Russian institute (Khavinson), with editor warnings about reliance on primary sources and undue weight; independent work only recently begun, focused on telomere length. Wikipedia, Epitalon.
Written by Viktor Lindqvist, medical writer. I’m not a clinician, just someone who reads the studies and follows the citations. Last reviewed January 2026.
Not medical advice, just context. A healthcare provider who knows your history should advise you.